
Purpose of This Guideline
Date of current publication: March 7, 2024
Lead author: James C. M. Brust, MD
Writing group: Joseph P. McGowan, MD, FACP, FIDSA; Steven M. Fine, MD, PhD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Rona M. Vail, MD; Brianna Norton, DO, MPH; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: June 30, 2017
This guideline was developed by the New York State Department of Health AIDS Institute (NYSDOH AI) for primary care providers and other practitioners who manage immune reconstitution inflammatory syndrome (IRIS) in patients with HIV. The guideline aims to achieve the following goals:
- Raise awareness among healthcare providers about IRIS, including its clinical presentation.
- Provide treatment recommendations for IRIS.
- Encourage clinicians to seek the assistance of an experienced HIV care provider when managing IRIS.
- Emphasize that antiretroviral therapy (ART) should not be interrupted in patients with IRIS except in life-threatening cases.
The NYSDOH AI is publishing this guideline at a critical time: 1) Initiation of ART is now recommended for all patients diagnosed with HIV; 2) Identifying and linking patients with HIV infection to care and treatment that achieves optimal virologic suppression are crucial to the success of New York State’s Ending the Epidemic initiative; and 3) The ability of primary care providers and other clinicians in New York State to manage IRIS is key to the successful treatment of patients with HIV.
Although ART dramatically reduces HIV-associated mortality and improves patient outcomes, initiation of or a change in ART introduces the potential for IRIS. This early complication is seen most often within the first 8 weeks of therapy in patients with advanced HIV disease. Mild IRIS resolves over time in most patients, and symptomatic treatment is often sufficient. Severe IRIS may threaten a patient’s functional status or cause permanent disability or death. But interrupting combination ART in a patient with IRIS may lead to acquisition of new opportunistic infections, recurrence of IRIS when therapy is later restarted, and possible HIV-drug resistance.
This guideline, therefore, addresses management of IRIS to avoid ART interruption except in life-threatening cases. Key recommendations cover the following:
- Timing of ART initiation relative to timing of treatment for opportunistic infections
- When to consult an experienced HIV care provider
- Diagnosis of IRIS
- Management and treatment of mild and severe IRIS
Note on “experienced” and “expert” HIV care providers: Throughout this guideline, when reference is made to “experienced HIV care provider” or “expert HIV care provider,” those terms are referring to the following 2017 NYSDOH AI definitions:
- Experienced HIV care provider: Practitioners who have been accorded HIV Experienced Provider status by the American Academy of HIV Medicine or have met the HIV Medicine Association’s definition of an experienced provider are eligible for designation as an HIV Experienced Provider in New York State. Nurse practitioners and licensed midwives who provide clinical care to individuals with HIV in collaboration with a physician may be considered HIV Experienced Providers as long as all other practice agreements are met (8 NYCRR 79-5:1; 10 NYCRR 85.36; 8 NYCRR 139-6900). Physician assistants who provide clinical care to individuals with HIV under the supervision of an HIV Specialist physician may also be considered HIV Experienced Providers (10 NYCRR 94.2)
- Expert HIV care provider: A provider with extensive experience in the management of complex patients with HIV.
Manifestations of IRIS
The goal of antiretroviral therapy (ART) in individuals with HIV is immune reconstitution, which may also produce the manifestation of immune reconstitution inflammatory syndrome (IRIS). IRIS, which is also known as immune restoration disease, refers to a disease- or pathogen-specific inflammatory response that may be triggered after ART initiation in treatment-naive patients, after re-initiation of ART, or after a change to a more effective ART regimen in patients who fail to achieve viral suppression. After a patient starts ART, IRIS may manifest as a worsening of previously diagnosed disease, termed paradoxical IRIS, or as the appearance of a previously undiagnosed disease, termed unmasking IRIS.
| TERMINOLOGY |
|
IRIS is usually accompanied by an increase in CD4 count and/or a rapid decrease in viral load. Although most cases of IRIS occur in patients who have low CD4 counts and high viral loads at the time of ART initiation, IRIS can occur at any CD4 count Breton, et al. 2004; Shelburne(a), et al. 2005; Shelburne(b), et al. 2005; Müller, et al. 2010; Novak, et al. 2012. It usually presents within the first 4 to 8 weeks after ART initiation but has occurred many weeks later and in sequestered sites, such as bone McComsey, et al. 2012.
Development and Pathogenesis of IRIS
IRIS often presents within the first 4 to 8 weeks after initiation of or a change in ART as mild to moderate disease or symptoms; life-threatening cases are rare Müller, et al. 2010. Although most cases of IRIS occur in patients who, at the time of ART initiation, have a low CD4 count, particularly below 50 cells/mm3, and a high viral load (>100,000 copies/mL) Breton, et al. 2004; Shelburne(a), et al. 2005; Shelburne(b), et al. 2005; Müller, et al. 2010; Novak, et al. 2012, specific changes in these markers are not required for the diagnosis of IRIS. For example, IRIS may occur without a significant increase in the absolute CD4 count, suggesting that measurements obtained from the peripheral blood may not reflect the number of CD4 cells present at the site of an opportunistic infection (OI) Haddow(b), et al. 2010. Some studies have found a higher incidence of IRIS in patients treated with regimens containing integrase strand transfer inhibitors (INSTIs), which was hypothesized to be related to the rapid drop in viral load associated with INSTI treatment Wijting, et al. 2019; Dutertre, et al. 2017; Psichogiou, et al. 2017. A meta-analysis of 14 randomized controlled trials including more than 8,500 participants did not, however, find any difference in risk of IRIS between those receiving versus not receiving integrase inhibitors Zhao, et al. 2022.
Although understanding of the pathogenesis of IRIS, including the inflammatory role of T-regulatory cells and cytokine imbalances Shankar, et al. 2008; Boulware(a), et al. 2010; Haddow(a), et al. 2010, remains largely speculative, inflammatory reactions to many pathogens have been described, including mycobacteria, fungi, viruses, and bacteria (see Table 2: Major and Minor Presentations of IRIS). IRIS that involves worsening symptoms of some malignancies, including Kaposi’s sarcoma (KS) Feller, et al. 2008, and autoimmune phenomena, such as sarcoid Foulon, et al. 2004, also have been documented. IRIS may be more severe in patients with a higher burden of an OI organism, suggesting that antigen load may play a role in pathogenesis Shelburne(a), et al. 2005.
Paradoxical IRIS
“Paradoxical IRIS” describes the worsening of previously diagnosed disease after ART is initiated. Epidemiologic data regarding paradoxical IRIS are variable and depend largely on the CD4 count and the prevalence and types of OI present at the time of ART initiation. A review and meta-analysis of 54 cohort studies from 22 countries that included 13,903 patients initiating ART found that, overall, 13% of patients developed IRIS Müller, et al. 2010. In 22 studies (41%) that reported participants’ CD4 counts at the start of therapy, CD4 counts were low overall, with a median of 57 cells/mm3 (range, 17 to 174 cells/mm3), and occurrences of IRIS were significantly higher among patients with CD4 counts <50 cells/mm3. Though rates of IRIS were highest in patients with cytomegalovirus (CMV) retinitis (37.7%), it was also observed in patients with cryptococcal meningitis (19.5%), progressive multifocal leukoencephalopathy (16.7%), tuberculosis (TB) (15.7%), herpes zoster (12.2%), and KS (6.4%). As noted in the analysis, the higher occurrences of IRIS associated with CMV retinitis, in particular, were not surprising because this condition most often occurs at CD4 counts <50 cells/mm3. Significant heterogeneity between studies was also noted, in part, because of non-standardized diagnostic criteria and difficulty in distinguishing IRIS from the progression of OIs.
In the United States, the prospective AIDS Clinical Trials Group study A5164 reported IRIS in 7.6% of patients Grant, et al. 2010, and another large multisite U.S. prospective cohort reported an occurrence of 10.6% Novak, et al. 2012.
However, concurrent steroid treatment in some individuals and the studies’ inclusion of low numbers of patients with the OIs that are most commonly associated with IRIS may obscure the true incidence. Retrospective studies have reported a higher occurrence, with IRIS reported in 63% of patients with a history of CMV retinitis Karavellas, et al. 1999 and in 30% to 34% of those with previously diagnosed cryptococcal infection Shelburne(a), et al. 2005; Shelburne(b), et al. 2005. Other retrospective studies have reported IRIS in 30% and 31% of patients with TB and Mycobacterium avium complex (MAC), respectively Shelburne(b), et al. 2005. However, the studies were conducted in the era before early treatment, when ART was more often initiated in patients with low CD4 counts, and, as retrospective studies, are more likely to overestimate the incidence of IRIS.
Unmasking IRIS
“Unmasking IRIS” describes the appearance of previously undiagnosed disease after ART is initiated. Data on unmasking IRIS are limited primarily to case reports. A re-analysis of cohort data from 6 European countries and the United States found a significantly increased risk of MAC-IRIS up to 3 months after ART initiation. A slight but statistically nonsignificant increase of IRIS-associated TB, CMV retinitis, herpes simplex virus, KS, and non-Hodgkin lymphoma was reported among patients without HIV who had a median CD4 count of 279 cells/mm3 at the time of ART initiation. The epidemiologic patterns for MAC and TB were most consistent with unmasking IRIS Lodi, et al. 2014. In a French study of 47 patients taking ART at the time of TB diagnosis, 11 patients were diagnosed with unmasking TB-IRIS; identified risk factors for unmasking TB-IRIS included African origin, higher baseline RNA, and a strong response to ART Valin, et al. 2010.
Mortality
IRIS is associated with an increased risk of death, with a reported overall mortality rate of 4.5% Müller, et al. 2010; Novak, et al. 2012. However, mortality rates depend on the associated OI, access to treatment, diagnostic criteria, degree of immunosuppression, and geography. In general, the highest mortality rates (13% to 75%) have been reported among patients with IRIS affecting the central nervous system Müller, et al. 2010; Bahr, et al. 2013.
Timing of ART Initiation in Patients with Recent OIs and Prevention of IRIS
| RECOMMENDATIONS |
Initiating ART
Pulmonary TB
TB Meningitis or Extrapulmonary TB
Cryptococcal Meningitis
CMV Retinitis
|
Abbreviations: ART, antiretroviral therapy; CMV, cytomegalovirus; HBV, hepatitis B virus; HCV, hepatitis C virus; IRIS, immune reconstitution inflammatory syndrome; OI, opportunistic infection; TB, tuberculosis. |
Initiating ART
Because ART is key to the recovery of immune function, the benefits of early ART initiation outweigh the risks of IRIS under most circumstances Ford, et al. 2018; Lodi, et al. 2014; Grant, et al. 2010. Clinicians should strongly recommend that patients being treated for any of the following active infections initiate ART within 2 weeks of starting OI treatment or as soon as the patient is clinically stable on OI therapy and the potential for drug-drug interactions has been minimized:
- Cryptosporidiosis
- Microsporidiosis
- Progressive multifocal leukoencephalopathy
- Kaposi’s sarcoma (KS)
- Pneumocystis jiroveci pneumonia—formerly known as Pneumocystis carinii
- HBV infection
- HCV infection
- Any other serious bacterial infection
The optimal timing for ART initiation is not well established for other OIs, including TB meningitis, extrapulmonary TB, CMV retinitis, and cryptococcal meningitis, as described below. Clinicians should consult with a care provider experienced in the management of ART in patients with these infections.
| KEY POINTS |
|
| Abbreviations: ART, antiretroviral therapy; OI, opportunistic infection; TB, tuberculosis. | |
| Table 1: Summary of Recommendations Regarding Timing of ART Initiation | |
| Opportunistic Infection | Timing of ART Initiation After Starting OI Treatments |
|
Within 2 weeks of starting treatment for an OI or as soon as the patient is clinically stable. |
| Pulmonary TB |
|
| Extrapulmonary TB | Optimal timing has not been established; consult with an experienced HIV care provider. |
| TB meningitis | Optimal timing has not been established; consult with an experienced HIV care provider. |
| Cryptococcal meningitis |
|
| Cryptococcal infection other than meningitis |
|
| Cytomegalovirus retinitis |
|
Prevention of complications associated with IRIS involves careful monitoring, particularly in patients with low CD4 counts and past or current history of co-infections. After initiating ART in patients at the highest risk for IRIS, including those with CD4 counts <100 cells/mm3 or known concomitant OIs, clinicians should be vigilant for signs and symptoms of IRIS, which are described in more detail in the guideline section Presentation and Diagnosis of IRIS. These patients should be counseled about the risk of developing IRIS at the time of ART initiation. To promote trust in the treatment plan and adherence to ART, patients should be informed that starting ART could lead to an initial worsening of OI symptoms or the appearance of a previously undiagnosed OI (e.g., herpes zoster).
Pulmonary TB
Immune reconstitution inflammatory syndrome (IRIS) has been described in 8% to 51% of patients with HIV and TB after initiation of ART Meintjes, et al. 2008; Haddow(b), et al. 2010; Narendran, et al. 2013 with a reported overall mortality rate of 2% Namale, et al. 2015. In determining the timing of ART initiation in patients with HIV/TB co-infection, the risk of TB-IRIS and the overlapping toxicity, potential drug-drug interactions, and adherence challenges of multidrug therapy for HIV and TB warrant careful consideration.
Several studies have assessed the optimal timing of ART initiation during treatment for pulmonary TB Amogne, et al. 2015; Mfinanga, et al. 2014; Manosuthi, et al. 2012; Sinha, et al. 2012; Blanc, et al. 2011; Havlir, et al. 2011; Abdool Karim, et al. 2010. Two separate meta-analyses compared ART initiation at 1 to 4 weeks after starting TB treatment with ART initiation at >4 weeks after starting TB treatment. Both studies found a statistically significant decrease in mortality with early ART initiation only in the subgroup of patients with CD4 counts <50 cells/mm3. Early ART reduced the incidence of AIDS-defining events but nearly doubled the incidence of TB-IRIS irrespective of CD4 count Burke, et al. 2021; Uthman, et al. 2015. The authors concluded that although early ART improves survival for patients with low CD4 counts, not enough evidence is available to support or refute a survival benefit from early ART in patients with pulmonary TB who have CD4 counts >50 cells/mm3 Uthman, et al. 2015. Further studies are needed to more definitively determine the CD4 count threshold below which the mortality benefit supports early initiation of ART.
Two trials compared ART initiation during TB treatment with deferral until after completion of TB treatment. The SAPIT trial (n = 642) in South Africa Abdool Karim, et al. 2010, which evaluated patients with smear-positive TB, was stopped early because the mortality rate in the group that initiated ART during TB treatment was 56% lower than in the deferred group. The survival benefit of initiating ART before completing TB treatment was observed in all ranges of CD4 counts but was highest in patients with CD4 counts <50 cells/mm3. Although the incidence of IRIS was much higher in patients who initiated ART early, it was mostly mild and was outweighed by the other benefits of early treatment. The subsequent TB- HAART trial (n = 1,675), conducted in South Africa, Tanzania, Uganda, and Zambia Mfinanga, et al. 2014, compared initiation of ART after 2 weeks of TB treatment with ART initiation deferred until after completion of 6 months of TB treatment in patients with CD4 counts >220 cells/mm3. More grade 3 and 4 adverse events were reported among those with early ART initiation, with no difference in mortality or IRIS incidence between early and deferred ART.
Although early ART increases the risk of TB-associated IRIS, this risk should be weighed against the survival benefit of early HIV treatment given a patient’s CD4 count. The benefits of early ART initiation in patients with active TB and very low CD4 counts (<50 cells/mm3) likely outweigh the risks for morbidity associated with TB-IRIS Lawn, et al. 2007; Battegay, et al. 2008. To decrease the risk of IRIS, initiation of ART may be safely delayed up to 12 weeks after starting TB therapy in patients with CD4 counts of ≥50 cells/mm3. Careful monitoring for IRIS, and timely treatment if it occurs, may significantly reduce morbidity associated with TB-IRIS; it may also ensure that other risks associated with severe immunosuppression (CD4 counts <50 cells/mm3) are managed effectively with ART.
A study of 240 patients enrolled in the PredART trial demonstrated that prednisone initiated around the time of ART initiation reduced the risk of IRIS in patients receiving TB treatment Meintjes, et al. 2018. ART-naive adults with HIV infection, CD4 counts <100 cells/mm3, who were on confirmed treatment for TB were randomized to receive either 40 mg per day of prednisone for 2 weeks followed by 20 mg per day of prednisone for 2 weeks or placebo. The prednisone and ART were initiated on the same day and were initiated within 30 days of the start of TB treatment. Use of corticosteroids was allowed to treat IRIS if it developed. Patients with rifampin resistance, central nervous system TB, Karposi’s sarcoma, hepatitis B surface antigen positive, or poor adherence were excluded from the study. In patients receiving prednisone, TB-IRIS was reduced by 30% (47% vs 33%; RR 0.7, p 0.03) and subsequent use of corticosteroids to treat IRIS was reduced by 53% (28% vs 13%; RR 0.47). Grade 3 adverse events were reduced from 45% to 28% (p 0.01), and fewer hospitalizations occurred in patients who received prednisone. The prednisone was well tolerated, and there were no additional infections or malignancies in patients receiving prednisone compared with those receiving placebo.
TB Meningitis and Extrapulmonary TB
Compared with non-central nervous system-related diseases, immune reconstitution inflammatory syndrome (IRIS)-associated TB meningitis has a higher mortality rate Marais, et al. 2013. The optimal timing of ART initiation in patients treated for TB meningitis or extrapulmonary TB remains unclear. In a randomized controlled trial, initiation of ART within 7 days was not associated with increased survival for patients with TB meningitis compared with delaying treatment for 2 months. Although the incidence of severe (grade 3 and 4) adverse events was similar in the 2 groups, early initiation of ART was associated with a higher incidence of the most severe (grade 4) adverse events Török, et al. 2011. A 2- to 9-fold increased risk of development of IRIS has been described for patients with extrapulmonary TB after ART initiation Namale, et al. 2015; however, insufficient data are available to guide timing of ART initiation.
Cryptococcal Meningitis
With rapid immune reconstitution in patients with cryptococcal meningitis, there is a risk of increased inflammatory response in the meninges that can lead to paradoxical worsening of the symptoms and, sometimes, death. Paradoxical IRIS was noted in 6% to 45% of patients with cryptococcal meningitis following ART initiation Longley, et al. 2013. Most cases occurred within the first 1 to 2 months, but some occurred 6 to 9 months later. The presentation of cryptococcal IRIS may mimic aseptic meningitis and can be difficult to distinguish from progression of cryptococcal disease associated with treatment failure Bicanic, et al. 2009; Boulware(b), et al. 2010; Haddow(a), et al. 2010.
| KEY POINTS |
|
The optimal timing of ART initiation in patients with cryptococcal meningitis is controversial, with inconclusive study results among the 4 trials conducted to date. In 2 studies (each with fewer than 40 participants with cryptococcal meningitis), initiation of ART within 2 weeks of diagnosis was observed to be safe but without significant improvement in survival Zolopa, et al. 2009; Bisson, et al. 2013. In contrast, 2 clinical trials were stopped early because of a high mortality rate in the early ART arm Makadzange, et al. 2010; Boulware, et al. 2014. In a study from Zimbabwe of 54 patients with cryptococcal meningitis, administration of ART within 72 hours of diagnosis resulted in higher mortality than when ART was deferred for 10 or more weeks Makadzange, et al. 2010. The more recent and larger COAT trial involving 177 ART-naive patients with HIV and cryptococcal meningitis in Uganda and South Africa was also stopped early because of a 15% higher mortality in the group randomized to ART initiation within 2 weeks compared with delaying treatment by at least 5 weeks Boulware, et al. 2014. However, interpretation of results is limited because neither trial included flucytosine in the cryptococcal treatment regimen Scriven, et al. 2015.
Until further studies are available to definitively determine the optimal time for ART initiation for patients with cryptococcal meningitis, treatment should be delayed for at least 2 weeks (after completion of antifungal therapy induction phase) and possibly for up to 10 weeks (after completion of both induction and consolidation phases of antifungal therapy), particularly in those with increased intracranial pressure or low cerebral spinal fluid white blood cell counts. If ART is started before 10 weeks, clinicians should be vigilant for signs and symptoms of IRIS and aggressively manage any complications. The optimal timing for initiation of ART for other forms of cryptococcosis is also unclear; it is recommended to delay ART initiation for at least 2 weeks after starting antifungal therapy DHHS 2021.
CMV Retinitis
Immediate initiation of ART is not recommended based on the results of a controlled study that reported a lower prevalence and severity of immune recovery uveitis in patients with deferred initiation of ART Ortega-Larrocea, et al. 2005. The optimal timing for initiation of ART in patients treated for CMV retinitis has not been definitively established. The overall incidence of CMV-IRIS has declined to an estimated 2.7 to 3.6 per 100 person-years in recent years Jabs, et al. 2010; Jabs, et al. 2015, and the risk of IRIS should be weighed against the risk of developing other OIs due to delay in ART initiation.
To avoid the possible devastating effects of CMV-IRIS, ART should not be started immediately in patients with known or strongly suspected CMV. All patients with HIV who have CD4 counts <100 cells/mm3 who do not have known or strongly suspected CMV should be screened for signs of CMV by dilated ophthalmologic examination as soon as possible after initiation of ART. If signs of CMV are seen on dilated exam, clinicians should consult with an experienced HIV care provider to determine if ART must be temporarily paused. In mild cases, it may be appropriate to continue ART while treating the CMV, but such patients must be followed closely by an ophthalmologist with experience in managing CMV retinitis.
Even if receiving treatment, patients with a history of CMV retinitis should receive a dilated ophthalmologic examination every 3 months for the first year after initiation of ART and immediately if there is a change in visual acuity or development of floaters. Cases of CMV-IRIS myelopathy that respond to steroids have been reported, as have cases of CMV-IRIS colitis Acosta, et al. 2008; von Both, et al. 2008. For more information, see DHHS: Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV > Cytomegalovirus Disease.
Presentation and Diagnosis of IRIS
| RECOMMENDATIONS |
Diagnosing IRIS
|
Abbreviations: ART, antiretroviral therapy; IRIS, immune reconstitution inflammatory syndrome. |
Table 2, below, describes major and minor clinical presentations of IRIS. Proposed case definitions do not provide clear consensus on the many manifestations of IRIS French, et al. 2004; Robertson, et al. 2006; Shelburne, et al. 2006; Meintjes, et al. 2008; Bicanic, et al. 2009; Haddow(a), et al. 2010; Haddow(b), et al. 2010. Common features are clinical deterioration after ART initiation and localized tissue inflammation, with or without a systemic inflammatory response Walker, et al. 2015, but the presentation of IRIS varies depending on the underlying opportunistic infection (OI) or illness. The majority of IRIS cases occur within 4 to 8 weeks after initiation of or a change in ART Breton, et al. 2004; Shelburne(a), et al. 2005; Novak, et al. 2012. However, cases have been reported as early as 3 days or as late as several months, or, rarely, several years, after ART initiation Rambeloarisoa, et al. 2002; Lortholary, et al. 2005; Shelburne(b), et al. 2005; Haddow(b), et al. 2010; Valin, et al. 2010; Novak, et al. 2012; Letang, et al. 2013. Late manifestations of IRIS (>7 months) may be atypical, such as osteomyelitis resulting from Mycobacterium avium complex Aberg, et al. 2002.
A definitive diagnostic test is not available for IRIS; therefore, diagnosis is based largely on clinical judgment, which may be challenged by the broad array of IRIS signs and symptoms and the presence of multiple OIs. A rise in CD4 count is often present in IRIS cases but is not a required criterion for diagnosis Robertson, et al. 2006; Meintjes, et al. 2008; Haddow(a), et al. 2010; Haddow(b), et al. 2010; Walker, et al. 2015; therefore, absence of an increase in absolute CD4 count should not exclude the possibility of IRIS during a paradoxical response to treatment of an OI.
In patients who were responding favorably to OI treatment prior to ART initiation, but who worsen after, the differential diagnosis includes paradoxical IRIS, OI treatment toxicity, OI drug resistance, poor OI treatment adherence, or development of a new OI. Development of a new OI after ART initiation of ART may be attributable to unmasking IRIS or to the effects of persistent immune compromise Walker, et al. 2015.
| Abbreviations: ART, antiretroviral therapy; IRIS, immune reconstitution inflammatory syndrome; MRI, magnetic resonance imaging. | |
| Table 2: Major and Minor Presentations of IRIS | |
| Underlying Opportunistic Infection | IRIS Signs/Symptoms |
| Major Presentations | |
| Tuberculosis (TB) |
|
| Mycobacterium avium complex (MAC) |
|
| Cryptococcal meningitis | Usually presents as worsening of meningitis symptoms Rambeloarisoa, et al. 2002; Gray, et al. 2005; Lawn(b), et al. 2005; Lortholary, et al. 2005; Shelburne(a), et al. 2005; Kambugu, et al. 2008, including possible rapid hearing and/or vision loss, ataxia, and/or elevated intracranial pressure. |
| Cytomegalovirus (CMV) retinitis |
|
| Hepatitis B or C virus |
|
| Progressive multifocal leukoencephalopathy (PML) | PML lesions may be unmasked or worsen and could appear as new or worsening focal neurologic deficits or lesions on MRI Summers, et al. 2019; Tan, et al. 2009; Gray, et al. 2005; Safdar, et al. 2002. |
| Kaposi’s sarcoma (KS) |
|
| Cerebral toxoplasmosis | May present as a cerebral abscess (also known as toxoplasmosis encephalitis) or, rarely, diffuse encephalitis or chorioretinitis Bowen, et al. 2016. |
| Histoplasmosis | May present as mucocutaneous lesions, disseminated disease, or fever without localizing symptoms Melzani, et al. 2020. |
| Autoimmune diseases |
|
| Minor Presentations | |
| Herpes simplex virus (HSV) and varicella zoster virus (VZV) |
|
| Mpox | Several case reports have described worsening of previously crusted lesions, the appearance of new lesions, and necrosis after ART initiation Martinez, et al. 2023; Rajme-López, et al. 2023; Warner, et al. 2023. |
| Nonspecific dermatologic complications | A number of dermatologic manifestations, such as folliculitis and oral and genital warts, may appear or worsen during immune reconstitution. |
Download Table 2: Major and Minor Presentations of IRIS Printable PDF
Management and Treatment of IRIS
| RECOMMENDATIONS |
Management and Treatment
Severe IRIS
|
Abbreviations: ART, antiretroviral therapy; CMV, cytomegalovirus; IRIS, immune reconstitution inflammatory syndrome; KS, Kaposi’s sarcoma; OI, opportunistic infection; TB, tuberculosis. |
Whenever IRIS is suspected, initial efforts should focus on diagnosing and treating the underlying OI. IRIS resolves over time in most patients, and if not severe, symptomatic treatment is often sufficient.
Mild IRIS
When minor IRIS presentations occur, clinicians can reassure patients that symptoms are an indication of immune reconstitution rather than progression of HIV disease and will resolve with standard treatment. In addition to standard therapy for the underlying OI to reduce pathogen load, the following treatments may alleviate inflammation in patients with mild IRIS:
- Nonsteroidal anti-inflammatory agents for discomfort associated with mild inflammation or fevers
- Drainage of abscesses
- Excision of inflamed and painful lymph nodes
- Inhaled steroids for bronchospasm or cough associated with mild pulmonary inflammation
Severe IRIS
Severe IRIS may threaten a patient’s functional status or may cause permanent disability. Examples of this are a decline in pulmonary capacity from TB or Mycobacterium avium complex (MAC) infection, neurologic complications from cryptococcal infection, or vision loss from CMV retinitis infection.
Corticosteroid therapy to suppress inflammatory response is the most commonly used intervention in cases of severe IRIS. Studies to determine the effectiveness of corticosteroid treatment are limited. A randomized, placebo-controlled trial demonstrated benefits of corticosteroids for paradoxical TB-IRIS Meintjes, et al. 2010, and a study of patients with MAC-IRIS (n = 9) demonstrated clinical response to prednisone Phillips, et al. 2005. No trials have compared different dosing regimens of corticosteroids, but this Committee recommends 1 to 2 mg/kg prednisone, or the equivalent, for 1 to 2 weeks, followed by a period of tapering dose that is individualized. If a flare of symptoms occurs during or at the end of the steroid taper, the dose may be increased and the taper slowed, and the patient should be assessed for possible disease progression due to failure of treatment.
The risks of corticosteroid therapy should be weighed against the severity of the IRIS manifestations and the potential benefits, particularly given the high prevalence of type 2 diabetes, hypertension, and mental health disorders among patients with HIV. Risks of corticosteroid therapy include the following:
- Hyperglycemia
- Hypertension
- Mental status changes
- Avascular necrosis
- Worsening of an existing infection
- Predisposition to a new infection
Except in the most severe cases, ART should not be interrupted in patients with IRIS. Discontinuation of ART can be considered in life-threatening cases in which corticosteroids did not result in improvement, usually associated with central nervous system (CNS)-IRIS. Risks of stopping combination ART include acquisition of new OIs and recurrence of IRIS when therapy is later restarted. HIV drug resistance may also be a theoretical concern. The decision to stop ART should be made in consultation with an experienced HIV care provider if possible.
| KEY POINT |
|
In cases of cryptococcal-IRIS with worsening meningitis symptoms, including cranial nerve defects, hearing, or vision changes, therapeutic lumbar puncture can be used to lower intracranial pressure. Corticosteroids are not recommended for treatment of cryptococcal meningitis in patients with HIV. A trial of treatment of HIV-associated cryptococcal meningitis with dexamethasone was stopped because of the high incidence of adverse events and disability observed in the treatment arm compared with placebo Beardsley, et al. 2016.
Corticosteroids are associated with increased risk of development of new KS or worsening of pre-existing disease among patients with HIV Gill, et al. 1989; Elliott, et al. 2004; Volkow, et al. 2008. Treatment of CMV vitritis with intraocular steroids has been described Schrier, et al. 2006 but has not been useful in uveitis.
There are limited case reports of improvement in clinical symptoms following treatment with thalidomide and other immunomodulators (pentoxifylline, chloroquine, TNF-a inhibitors, leukotriene antagonists) in patients with severe disease Armange, et al. 2023; Fourcade, et al. 2014; Brunel, et al. 2012; Meintjes, et al. 2012; Marais, et al. 2009; Hardwick, et al. 2006. However, data are insufficient to recommend the use of these alternative therapies.
The CCR5 inhibitor maraviroc has been used for treatment of progressive multifocal leukoencephalopathy-associated IRIS because direct treatment for JC virus is not available to lower the pathogen burden and treatment with corticosteroids may dampen the immune response. However, case reports indicate mixed success Martin-Blondel, et al. 2009; Giacomini, et al. 2014; Rodríguez, et al. 2014, and a recent randomized, placebo-controlled trial found that maraviroc was not effective for prevention of IRIS in patients starting ART with CD4 count <100 cells/mm3 and HIV RNA >1,000 copies/mL Sierra-Madero, et al. 2014.
For further OI-specific guidance on management of IRIS, see DHHS: Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV McComsey, et al. 2012.
All Recommendations
| ALL RECOMMENDATIONS: MANAGEMENT OF IRIS |
Initiating ART
Pulmonary TB
TB Meningitis or Extrapulmonary TB
Cryptococcal Meningitis
CMV Retinitis
Diagnosing IRIS
Management and Treatment
Severe IRIS
|
Abbreviations: ART, antiretroviral therapy; CMV, cytomegalovirus; HBV, hepatitis B virus; HCV, hepatitis C virus; IRIS, immune reconstitution inflammatory syndrome; KS, Kaposi’s sarcoma; OI, opportunistic infection; TB, tuberculosis. |
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
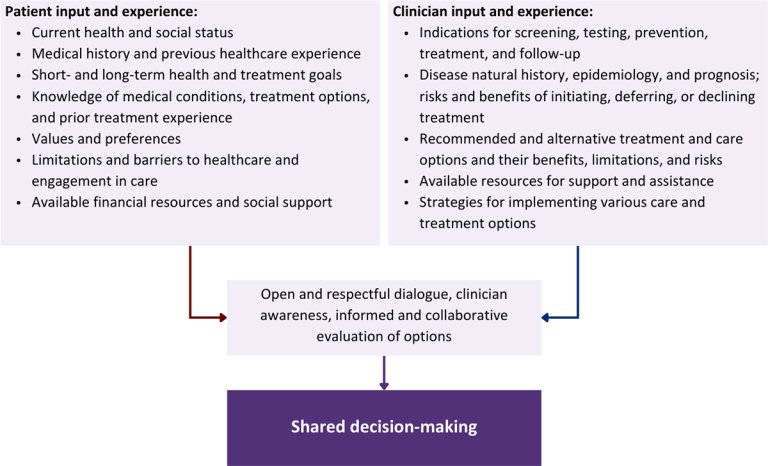
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
Download figure: Elements of Shared Decision-Making
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Abdool Karim S. S., Naidoo K., Grobler A., et al. Timing of initiation of antiretroviral drugs during tuberculosis therapy. N Engl J Med 2010;362(8):697-706. [PMID: 20181971]
Aberg J. A., Chin-Hong P. V., McCutchan A., et al. Localized osteomyelitis due to mycobacterium avium complex in patients with human immunodeficiency virus receiving highly active antiretroviral therapy. Clin Infect Dis 2002;35(1):E8-13. [PMID: 12060894]
Acosta R. D., Mays B. C., Wong R. K. Electronic clinical challenges and images in GI. CMV colitis with immune reconstitution syndrome. Gastroenterology 2008;134(2):e1-2. [PMID: 18242197]
Amogne W., Aderaye G., Habtewold A., et al. Efficacy and safety of antiretroviral therapy initiated one week after tuberculosis therapy in patients with CD4 counts < 200 cells/μL: TB-HAART Study, a randomized clinical trial. PLoS One 2015;10(5):e0122587. [PMID: 25966339]
Anderson A. M., Mosunjac M. B., Palmore M. P., et al. Development of fatal acute liver failure in HIV-HBV coinfected patients. World J Gastroenterol 2010;16(32):4107-11. [PMID: 20731028]
Armange L., Lacroix A., Petitgas P., et al. The use of TNF-. Eur J Clin Microbiol Infect Dis 2023;42(4):413-22. [PMID: 36795280]
Bahr N., Boulware D. R., Marais S., et al. Central nervous system immune reconstitution inflammatory syndrome. Curr Infect Dis Rep 2013;15(6):583-93. [PMID: 24173584]
Battegay M., Fehr J., Flückiger U., et al. Antiretroviral therapy of late presenters with advanced HIV disease. J Antimicrob Chemother 2008;62(1):41-44. [PMID: 18408235]
Beardsley J., Wolbers M., Kibengo F. M., et al. Adjunctive dexamethasone in HIV-associated cryptococcal meningitis. N Engl J Med 2016;374(6):542-54. [PMID: 26863355]
Bicanic T., Meintjes G., Rebe K., et al. Immune reconstitution inflammatory syndrome in HIV-associated cryptococcal meningitis: a prospective study. J Acquir Immune Defic Syndr 2009;51(2):130-34. [PMID: 19365271]
Bisson G. P., Molefi M., Bellamy S., et al. Early versus delayed antiretroviral therapy and cerebrospinal fluid fungal clearance in adults with HIV and cryptococcal meningitis. Clin Infect Dis 2013;56(8):1165-73. [PMID: 23362285]
Blanc F. X., Sok T., Laureillard D., et al. Earlier versus later start of antiretroviral therapy in HIV-infected adults with tuberculosis. N Engl J Med 2011;365(16):1471-81. [PMID: 22010913]
Boulware D. R., Meya D. B., Muzoora C., et al. Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. N Engl J Med 2014;370(26):2487-98. [PMID: 24963568]
Boulware(a) D. R., Meya D. B., Bergemann T. L., et al. Clinical features and serum biomarkers in HIV immune reconstitution inflammatory syndrome after cryptococcal meningitis: a prospective cohort study. PLoS Med 2010;7(12):e1000384. [PMID: 21253011]
Boulware(b) D. R., Bonham S. C., Meya D. B., et al. Paucity of initial cerebrospinal fluid inflammation in cryptococcal meningitis is associated with subsequent immune reconstitution inflammatory syndrome. J Infect Dis 2010;202(6):962-70. [PMID: 20677939]
Bowen L. N., Smith B., Reich D., et al. HIV-associated opportunistic CNS infections: pathophysiology, diagnosis and treatment. Nat Rev Neurol 2016;12(11):662-74. [PMID: 27786246]
Bower M., Nelson M., Young A. M., et al. Immune reconstitution inflammatory syndrome associated with Kaposi's sarcoma. J Clin Oncol 2005;23(22):5224-28. [PMID: 16051964]
Breton G., Duval X., Estellat C., et al. Determinants of immune reconstitution inflammatory syndrome in HIV type 1-infected patients with tuberculosis after initiation of antiretroviral therapy. Clin Infect Dis 2004;39(11):1709-12. [PMID: 15578375]
Brunel A. S., Reynes J., Tuaillon E., et al. Thalidomide for steroid-dependent immune reconstitution inflammatory syndromes during AIDS. AIDS 2012;26(16):2110-12. [PMID: 22874513]
Burke R. M., Rickman H. M., Singh V., et al. What is the optimum time to start antiretroviral therapy in people with HIV and tuberculosis coinfection? A systematic review and meta-analysis. J Int AIDS Soc 2021;24(7):e25772. [PMID: 34289243]
Crane M., Oliver B., Matthews G., et al. Immunopathogenesis of hepatic flare in HIV/hepatitis B virus (HBV)-coinfected individuals after the initiation of HBV-active antiretroviral therapy. J Infect Dis 2009;199(7):974-81. [PMID: 19231993]
DHHS. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: cryptococcosis. 2021 Jul 1. https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection/cryptococcosis?view=full [accessed 2021 Mar 8]
Drake A., Mijch A., Sasadeusz J. Immune reconstitution hepatitis in HIV and hepatitis B coinfection, despite lamivudine therapy as part of HAART. Clin Infect Dis 2004;39(1):129-32. [PMID: 15206064]
Dutertre M., Cuzin L., Demonchy E., et al. Initiation of antiretroviral therapy containing integrase inhibitors increases the risk of IRIS requiring hospitalization. J Acquir Immune Defic Syndr 2017;76(1):e23-26. [PMID: 28418992]
Elliott A. M., Luzze H., Quigley M. A., et al. A randomized, double-blind, placebo-controlled trial of the use of prednisolone as an adjunct to treatment in HIV-1-associated pleural tuberculosis. J Infect Dis 2004;190(5):869-78. [PMID: 15295690]
Feller L., Anagnostopoulos C., Wood N. H., et al. Human immunodeficiency virus-associated Kaposi sarcoma as an immune reconstitution inflammatory syndrome: a literature review and case report. J Periodontol 2008;79(2):362-68. [PMID: 18251652]
Ford N., Migone C., Calmy A., et al. Benefits and risks of rapid initiation of antiretroviral therapy. Aids 2018;32(1):17-23. [PMID: 29112073]
Foulon G., Wislez M., Naccache J. M., et al. Sarcoidosis in HIV-infected patients in the era of highly active antiretroviral therapy. Clin Infect Dis 2004;38(3):418-25. [PMID: 14727215]
Fourcade C., Mauboussin J. M., Lechiche C., et al. Thalidomide in the treatment of immune reconstitution inflammatory syndrome in HIV patients with neurological tuberculosis. AIDS Patient Care STDS 2014;28(11):567-69. [PMID: 25285462]
French M. A., Price P., Stone S. F. Immune restoration disease after antiretroviral therapy. AIDS 2004;18(12):1615-27. [PMID: 15280772]
Giacomini P. S., Rozenberg A., Metz I., et al. Maraviroc and JC virus-associated immune reconstitution inflammatory syndrome. N Engl J Med 2014;370(5):486-88. [PMID: 24476450]
Gill P. S., Loureiro C., Bernstein-Singer M., et al. Clinical effect of glucocorticoids on Kaposi sarcoma related to the acquired immunodeficiency syndrome (AIDS). Ann Intern Med 1989;110(11):937-40. [PMID: 2719427]
Grant P. M., Komarow L., Andersen J., et al. Risk factor analyses for immune reconstitution inflammatory syndrome in a randomized study of early vs. deferred ART during an opportunistic infection. PLoS One 2010;5(7):e11416. [PMID: 20617176]
Gray F., Bazille C., Adle-Biassette H., et al. Central nervous system immune reconstitution disease in acquired immunodeficiency syndrome patients receiving highly active antiretroviral treatment. J Neurovirol 2005;11 Suppl 3:16-22. [PMID: 16540449]
Haddow(a) L. J., Colebunders R., Meintjes G., et al. Cryptococcal immune reconstitution inflammatory syndrome in HIV-1-infected individuals: proposed clinical case definitions. Lancet Infect Dis 2010;10(11):791-802. [PMID: 21029993]
Haddow(b) L. J., Moosa M. Y., Easterbrook P. J. Validation of a published case definition for tuberculosis-associated immune reconstitution inflammatory syndrome. AIDS 2010;24(1):103-8. [PMID: 19926965]
Hardwick C., White D., Morris E., et al. Montelukast in the treatment of HIV associated immune reconstitution disease. Sex Transm Infect 2006;82(6):513-14. [PMID: 17151039]
Havlir D. V., Kendall M. A., Ive P., et al. Timing of antiretroviral therapy for HIV-1 infection and tuberculosis. N Engl J Med 2011;365(16):1482-91. [PMID: 22010914]
Jabs D. A., Ahuja A., Van Natta M., et al. Course of cytomegalovirus retinitis in the era of highly active antiretroviral therapy: five-year outcomes. Ophthalmology 2010;117(11):2152-61.e1-2. [PMID: 20673591]
Jabs D. A., Ahuja A., Van Natta M. L., et al. Long-term outcomes of cytomegalovirus retinitis in the era of modern antiretroviral therapy: results from a United States cohort. Ophthalmology 2015;122(7):1452-63. [PMID: 25892019]
Kambugu A., Meya D. B., Rhein J., et al. Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy. Clin Infect Dis 2008;46(11):1694-1701. [PMID: 18433339]
Karavellas M. P., Plummer D. J., Macdonald J. C., et al. Incidence of immune recovery vitritis in cytomegalovirus retinitis patients following institution of successful highly active antiretroviral therapy. J Infect Dis 1999;179(3):697-700. [PMID: 9952380]
Konopnicki D., Mocroft A., de Wit S., et al. Hepatitis B and HIV: prevalence, AIDS progression, response to highly active antiretroviral therapy and increased mortality in the EuroSIDA cohort. AIDS 2005;19(6):593-601. [PMID: 15802978]
Lawn S. D., Myer L., Bekker L. G., et al. Tuberculosis-associated immune reconstitution disease: incidence, risk factors and impact in an antiretroviral treatment service in South Africa. AIDS 2007;21(3):335-41. [PMID: 17255740]
Lawn S. D., Wood R. Hepatic involvement with tuberculosis-associated immune reconstitution disease. AIDS 2007;21(17):2362-63. [PMID: 18090294]
Lawn(a) S. D., Bekker L. G., Myer L., et al. Cryptococcocal immune reconstitution disease: a major cause of early mortality in a South African antiretroviral programme. AIDS 2005;19(17):2050-52. [PMID: 16260920]
Lawn(b) S. D., Bekker L. G., Miller R. F. Immune reconstitution disease associated with mycobacterial infections in HIV-infected individuals receiving antiretrovirals. Lancet Infect Dis 2005;5(6):361-73. [PMID: 15919622]
Leidner R. S., Aboulafia D. M. Recrudescent Kaposi's sarcoma after initiation of HAART: a manifestation of immune reconstitution syndrome. AIDS Patient Care STDS 2005;19(10):635-44. [PMID: 16232048]
Letang E., Lewis J. J., Bower M., et al. Immune reconstitution inflammatory syndrome associated with Kaposi sarcoma: higher incidence and mortality in Africa than in the UK. AIDS 2013;27(10):1603-13. [PMID: 23462220]
Lodi S., del Amo J., Moreno S., et al. Opportunistic infections and AIDS malignancies early after initiating combination antiretroviral therapy in high-income countries. AIDS 2014;28(16):2461-73. [PMID: 25265230]
Longley N., Harrison T. S., Jarvis J. N. Cryptococcal immune reconstitution inflammatory syndrome. Curr Opin Infect Dis 2013;26(1):26-34. [PMID: 23242412]
Lortholary O., Fontanet A., Mémain N., et al. Incidence and risk factors of immune reconstitution inflammatory syndrome complicating HIV-associated cryptococcosis in France. AIDS 2005;19(10):1043-49. [PMID: 15958835]
Makadzange A. T., Ndhlovu C. E., Takarinda K., et al. Early versus delayed initiation of antiretroviral therapy for concurrent HIV infection and cryptococcal meningitis in sub-saharan Africa. Clin Infect Dis 2010;50(11):1532-38. [PMID: 20415574]
Manosuthi W., Mankatitham W., Lueangniyomkul A., et al. Time to initiate antiretroviral therapy between 4 weeks and 12 weeks of tuberculosis treatment in HIV-infected patients: results from the TIME study. J Acquir Immune Defic Syndr 2012;60(4):377-83. [PMID: 22592586]
Marais S., Meintjes G., Pepper D. J., et al. Frequency, severity, and prediction of tuberculous meningitis immune reconstitution inflammatory syndrome. Clin Infect Dis 2013;56(3):450-60. [PMID: 23097584]
Marais S., Wilkinson R. J., Pepper D. J., et al. Management of patients with the immune reconstitution inflammatory syndrome. Curr HIV/AIDS Rep 2009;6(3):162-71. [PMID: 19589302]
Martin-Blondel G., Cuzin L., Delobel P., et al. Is maraviroc beneficial in paradoxical progressive multifocal leukoencephalopathy-immune reconstitution inflammatory syndrome management?. AIDS 2009;23(18):2545-46. [PMID: 19907215]
Martinez A. E., Frattaroli P., Vu C. A., et al. Successful outcome after treatment with cidofovir, vaccinia, and extended course of tecovirimat in a newly-diagnosed HIV patient with severe mpox: a case report. Vaccines (Basel) 2023;11(3):650. [PMID: 36992234]
McComsey G. A., Kitch D., Daar E. S., et al. Inflammation markers after randomization to abacavir/lamivudine or tenofovir/emtricitabine with efavirenz or atazanavir/ritonavir. AIDS 2012;26(11):1371-85. [PMID: 22546988]
Meintjes G., Lawn S. D., Scano F., et al. Tuberculosis-associated immune reconstitution inflammatory syndrome: case definitions for use in resource-limited settings. Lancet Infect Dis 2008;8(8):516-23. [PMID: 18652998]
Meintjes G., Rangaka M. X., Maartens G., et al. Novel relationship between tuberculosis immune reconstitution inflammatory syndrome and antitubercular drug resistance. Clin Infect Dis 2009;48(5):667-76. [PMID: 19191655]
Meintjes G., Scriven J., Marais S. Management of the immune reconstitution inflammatory syndrome. Curr HIV/AIDS Rep 2012;9(3):238-50. [PMID: 22752438]
Meintjes G., Stek C., Blumenthal L., et al. Prednisone for the prevention of paradoxical tuberculosis-associated IRIS. N Engl J Med 2018;379(20):1915-25. [PMID: 30428290]
Meintjes G., Wilkinson R. J., Morroni C., et al. Randomized placebo-controlled trial of prednisone for paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome. AIDS 2010;24(15):2381-90. [PMID: 20808204]
Melzani A., de Reynal de Saint Michel R., Ntab B., et al. Incidence and trends in immune reconstitution inflammatory syndrome associated with histoplasma capsulatum among people living with human immunodeficiency virus: a 20-year case series and literature review. Clin Infect Dis 2020;70(4):643-52. [PMID: 30921453]
Mfinanga S. G., Kirenga B. J., Chanda D. M., et al. Early versus delayed initiation of highly active antiretroviral therapy for HIV-positive adults with newly diagnosed pulmonary tuberculosis (TB-HAART): a prospective, international, randomised, placebo-controlled trial. Lancet Infect Dis 2014;14(7):563-71. [PMID: 24810491]
Müller M., Wandel S., Colebunders R., et al. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta-analysis. Lancet Infect Dis 2010;10(4):251-61. [PMID: 20334848]
Namale P. E., Abdullahi L. H., Fine S., et al. Paradoxical TB-IRIS in HIV-infected adults: a systematic review and meta-analysis. Future Microbiol 2015;10(6):1077-99. [PMID: 26059627]
Narendran G., Andrade B. B., Porter B. O., et al. Paradoxical tuberculosis immune reconstitution inflammatory syndrome (TB-IRIS) in HIV patients with culture confirmed pulmonary tuberculosis in India and the potential role of IL-6 in prediction. PLoS One 2013;8(5):e63541. [PMID: 23691062]
Novak R. M., Richardson J. T., Buchacz K., et al. Immune reconstitution inflammatory syndrome: incidence and implications for mortality. AIDS 2012;26(6):721-30. [PMID: 22233655]
Odongo F. C. Fatal disseminated Kaposi's sarcoma due to immune reconstitution inflammatory syndrome following HAART initiation. Case Rep Infect Dis 2013;2013:546578. [PMID: 23936695]
Ortega-Larrocea G., Espinosa E., Reyes-Terán G. Lower incidence and severity of cytomegalovirus-associated immune recovery uveitis in HIV-infected patients with delayed highly active antiretroviral therapy. AIDS 2005;19(7):735-38. [PMID: 15821403]
Perrella O., Sbreglia C., De Sena R., et al. Immune reconstitution: bad or good factor in hepatitis B virus and HIV co-infection?. AIDS 2006;20(5):790-91. [PMID: 16514319]
Phillips P., Bonner S., Gataric N., et al. Nontuberculous mycobacterial immune reconstitution syndrome in HIV-infected patients: spectrum of disease and long-term follow-up. Clin Infect Dis 2005;41(10):1483-97. [PMID: 16231262]
Psichogiou M., Basoulis D., Tsikala-Vafea M., et al. Integrase strand transfer inhibitors and the emergence of immune reconstitution inflammatory syndrome (IRIS). Curr HIV Res 2017;15(6):405-10. [PMID: 29173177]
Rajme-López S., Corral-Herrera E. A., Tello-Mercado A. C., et al. Clinical, molecular, and histological characteristics of severely necrotic and fatal mpox in HIV-infected patients. AIDS Res Ther 2023;20(1):85. [PMID: 38012656]
Rambeloarisoa J., Batisse D., Thiebaut J. B., et al. Intramedullary abscess resulting from disseminated cryptococcosis despite immune restoration in a patient with AIDS. J Infect 2002;44(3):185-88. [PMID: 12099747]
Rasul S., Delapenha R., Farhat F., et al. Graves' disease as a manifestation of immune reconstitution in HIV-infected individuals after initiation of highly active antiretroviral therapy. AIDS Res Treat 2011;2011:743597. [PMID: 21804938]
Robertson J., Meier M., Wall J., et al. Immune reconstitution syndrome in HIV: validating a case definition and identifying clinical predictors in persons initiating antiretroviral therapy. Clin Infect Dis 2006;42(11):1639-46. [PMID: 16652323]
Rodríguez M., Silva-Sánchez F. A., Luna-Rivero C., et al. Maraviroc failed to control progressive multifocal leukoencephalopathy-associated IRIS in a patient with advanced HIV infection. Case Rep Med 2014;2014:381480. [PMID: 25587282]
Safdar A., Rubocki R. J., Horvath J. A., et al. Fatal immune restoration disease in human immunodeficiency virus type 1-infected patients with progressive multifocal leukoencephalopathy: impact of antiretroviral therapy-associated immune reconstitution. Clin Infect Dis 2002;35(10):1250-57. [PMID: 12410486]
Schrier R. D., Song M. K., Smith I. L., et al. Intraocular viral and immune pathogenesis of immune recovery uveitis in patients with healed cytomegalovirus retinitis. Retina 2006;26(2):165-69. [PMID: 16467672]
Scriven J. E., Rhein J., Hullsiek K. H., et al. Early ART after cryptococcal meningitis is associated with cerebrospinal fluid pleocytosis and macrophage activation in a multisite randomized trial. J Infect Dis 2015;212(5):769-78. [PMID: 25651842]
Shankar E. M., Vignesh R., Velu V., et al. Does CD4+CD25+foxp3+ cell (Treg) and IL-10 profile determine susceptibility to immune reconstitution inflammatory syndrome (IRIS) in HIV disease?. J Inflamm (Lond) 2008;5:2. [PMID: 18282273]
Shelburne S. A., Montes M., Hamill R. J. Immune reconstitution inflammatory syndrome: more answers, more questions. J Antimicrob Chemother 2006;57(2):167-70. [PMID: 16354748]
Shelburne(a) S. A., Visnegarwala F., Darcourt J., et al. Incidence and risk factors for immune reconstitution inflammatory syndrome during highly active antiretroviral therapy. AIDS 2005;19(4):399-406. [PMID: 15750393]
Shelburne(b) S. A., Darcourt J., White A. C., et al. The role of immune reconstitution inflammatory syndrome in AIDS-related cryptococcus neoformans disease in the era of highly active antiretroviral therapy. Clin Infect Dis 2005;40(7):1049-52. [PMID: 15825000]
Sierra-Madero J. G., Ellenberg S. S., Rassool M. S., et al. Effect of the CCR5 antagonist maraviroc on the occurrence of immune reconstitution inflammatory syndrome in HIV (CADIRIS): a double-blind, randomised, placebo-controlled trial. Lancet HIV 2014;1(2):e60-67. [PMID: 26423989]
Sinha S., Shekhar R. C., Singh G., et al. Early versus delayed initiation of antiretroviral therapy for Indian HIV-Infected individuals with tuberculosis on antituberculosis treatment. BMC Infect Dis 2012;12:168. [PMID: 22846195]
Stover K. R., Molitorisz S., Swiatlo E., et al. A fatal case of Kaposi sarcoma due to immune reconstitution inflammatory syndrome. Am J Med Sci 2012;343(5):421-25. [PMID: 22227511]
Summers N. A., Kelley C. F., Armstrong W., et al. Not a disease of the past: a case series of progressive multifocal leukoencephalopathy in the established antiretroviral era. AIDS Res Hum Retroviruses 2019;35(6):544-52. [PMID: 30834775]
Tan K., Roda R., Ostrow L., et al. PML-IRIS in patients with HIV infection: clinical manifestations and treatment with steroids. Neurology 2009;72(17):1458-64. [PMID: 19129505]
Török M. E., Yen N. T., Chau T. T., et al. Timing of initiation of antiretroviral therapy in human immunodeficiency virus (HIV)--associated tuberculous meningitis. Clin Infect Dis 2011;52(11):1374-83. [PMID: 21596680]
Uthman O. A., Okwundu C., Gbenga K., et al. Optimal timing of antiretroviral therapy initiation for HIV-infected adults with newly diagnosed pulmonary tuberculosis: a systematic review and meta-analysis. Ann Intern Med 2015;163(1):32-39. [PMID: 26148280]
Valin N., Pacanowski J., Denoeud L., et al. Risk factors for 'unmasking immune reconstitution inflammatory syndrome' presentation of tuberculosis following combination antiretroviral therapy initiation in HIV-infected patients. AIDS 2010;24(10):1519-25. [PMID: 20549841]
Volkow P., Cesarman-Maus G., Garciadiego-Fossas P., et al. Clinical characteristics, predictors of immune reconstitution inflammatory syndrome and long-term prognosis in patients with Kaposi sarcoma. AIDS Res Ther 2017;14(1):30. [PMID: 28558783]
Volkow P., Cornejo P., Zinser J. W., et al. Life-threatening exacerbation of Kaposi's sarcoma after prednisone treatment for immune reconstitution inflammatory syndrome. AIDS 2008;22(5):663-65. [PMID: 18317012]
von Both U., Laffer R., Grube C., et al. Acute cytomegalovirus colitis presenting during primary HIV infection: an unusual case of an immune reconstitution inflammatory syndrome. Clin Infect Dis 2008;46(4):e38-40. [PMID: 18199043]
Walker N. F., Scriven J., Meintjes G., et al. Immune reconstitution inflammatory syndrome in HIV-infected patients. HIV AIDS (Auckl) 2015;7:49-64. [PMID: 25709503]
Warner N. C., Shishido A., Fulco P. P., et al. Immune reconstitution inflammatory syndrome due to monkeypox in two patients with AIDS. AIDS 2023;37(7):1187-88. [PMID: 37139659]
Wijting I. E. A., Wit F. W., Rokx C., et al. Immune reconstitution inflammatory syndrome in HIV infected late presenters starting integrase inhibitor containing antiretroviral therapy. EClinicalMedicine 2019;17:100210. [PMID: 31891143]
Zhao Y., Hohlfeld A., Namale P., et al. Risk of immune reconstitution inflammatory syndrome with integrase inhibitors versus other classes of antiretrovirals: a systematic review and meta-analysis of randomized trials. J Acquir Immune Defic Syndr 2022;90(2):232-39. [PMID: 35175970]
Zolopa A., Andersen J., Powderly W., et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: a multicenter randomized strategy trial. PLoS One 2009;4(5):e5575. [PMID: 19440326]
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | June 30, 2017 |
| Date of current publication | March 07, 2024 |
| Highlights of changes, additions, and updates in the March 07, 2024 edition |
|
| Intended users | Clinicians in New York State who are managing ART in patients with HIV and monitoring for and managing IRIS when indicated |
| Lead author |
James C. M. Brust, MD |
| Writing group |
Joseph P. McGowan, MD, FACP, FIDSA; Steven M. Fine, MD, PhD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Rona M. Vail, MD; Brianna Norton, DO, MPH; Charles J. Gonzalez, MD; Christopher J. Hoffmann, MD, MPH |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines | |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on July 30, 2024